5 Key Facts about Medicaid Program Integrity – Fraud, Waste, Abuse and Improper Payments
Medicaid is the primary program providing comprehensive coverage of health and long-term care to 83 million low-income people in the United States and accounts for one-fifth of health care spending. Medicaid is jointly financed by states and the federal government but administered by states within federal rules. The recently passed House budget resolution targets cuts to Medicaid of up to $880 billion or more over a decade. While several options appear to be under consideration to significantly reduce Medicaid spending, President Trump publicly said recently about Medicaid, “We are not going to touch it. Now, we are going to look for fraud.” Speaker Johnson has said, “Medicaid is hugely problematic because it has a lot of fraud, waste, and abuse.” Although fraud, waste, and abuse can be related concepts (and all fall under a broader “program integrity” umbrella), they are also distinct in important ways (Box 1). These terms apply to other government health care programs, private health insurance, and other government programs more broadly.1 On March 11, 2025, the White House released a statement saying most federal spending lost to fraud is from entitlement programs such as Medicaid and Medicare, citing “improper payment” estimates, without clarifying (as GAO does) that “improper payments” are not a measure of fraud or abuse and most improper payments are the result of missing documentation or missing administrative steps, and are not necessarily payments made for ineligible enrollees, providers, or services.
Speaker Johnson has referenced $50 billion in annual fraudulent payments (a figure that may reflect improper payments rather than fraud). In debates about broader Medicaid spending reductions, Republicans may try to recast policy changes such as adding work requirements to Medicaid and restricting the use of provider taxes as addressing fraud, waste, and abuse. Despite talk about eliminating fraud, the President’s recent order to remove Inspectors General (IGs), who are responsible for providing independent oversight of federal programs, from at least 17 government agencies—including HHS—appears to run counter to the stated focus on fraud, waste, and abuse. Recent KFF polling shows, while the public thinks that reducing fraud and waste in government health programs could lead to reductions in overall federal spending, many (60% of Republicans, 55% of Democrats, and 51% of independents) also think reducing fraud and waste in government programs could result in a reduction of benefits. Overall, most Americans (77%) hold favorable views of Medicaid, including six in ten Republicans (63%), and at least eight in ten independents (81%) and Democrats (87%).
This brief explains what is known about improper payments and fraud and abuse in Medicaid and describes ongoing state and federal actions to address program integrity.
Box 1: Definition of Terms
Fraud is the intentional act of deception and misrepresentation by a person with the knowledge that the deception could result in some unauthorized benefit to that person or another person (e.g., billing for services never provided). Medicaid fraud is generally considered a criminal act (42 CFR 433.304 and 455.2).
Abuse refers to provider practices that are inconsistent with acceptable business and medical practices (e.g., reimbursement for services that are not medically necessary or that don’t meet professionally recognized health care standards) that result in unnecessary cost to the program (42 CFR 455.2). It also includes beneficiary practices that result in unnecessary cost to the Medicaid program.
Waste is the inappropriate utilization of services and misuse of resources that result in unnecessary cost to the program (e.g., duplication of tests). Waste is not an intentional or criminal act.
Errors are mistakes made without intent or knowledge of the error.
Improper payments are any payments that should not have been made or that were made in an incorrect amount (including overpayments and underpayments) under statutory, contractual, administrative, or other requirements. It includes any payment to an ineligible recipient, any payment for an ineligible good or service, any duplicate payment, any payment for a good or service not received, and any payment that does not account for credit for applicable discounts (31 U.S.C. § 3351(4)). Office of Management and Budget (OMB) guidance instructs agencies to report as improper payments any payments for which insufficient or no documentation was found (31 U.S.C. § 3352(c)(2)).
1. Both the federal government and states are responsible for ensuring program integrity.
Program integrity refers to the proper management and functioning of the Medicaid program to ensure it is providing quality and efficient care while using funds–taxpayer dollars–appropriately with minimal waste. Medicaid is a very complex program that involves millions of beneficiaries, hundreds of thousands of providers, and significant federal and state expenditures. Program integrity efforts work to prevent and detect waste, fraud, and abuse, to increase program transparency and accountability, and to recover improperly used funds. Program integrity activities help ensure that eligibility decisions are made correctly; prospective and enrolled providers meet federal and state participation requirements; services provided to enrollees are medically necessary and appropriate; and provider payments are made in the correct amount and for appropriate services. Program integrity also includes routine oversight to ensure compliance with state and federal law.
State Medicaid agencies administer Medicaid on a day-to-day basis and have the primary responsibility for program integrity. Program integrity includes specific, dedicated activities, as well as activities that are built into program functions (e.g., beneficiary and provider enrollment, service delivery, payment). Federal laws and regulations include requirements for states to reduce fraud, waste, and abuse. Each state must have a Medicaid Fraud Control Unit (MFCU) to investigate fraud and prosecute or refer to prosecution individuals or entities defrauding Medicaid. Other state agencies and fiscal officers may be involved, including state auditors. Comprehensive managed care is the primary Medicaid delivery system (accounting for 75% of beneficiaries and over 50% of total Medicaid spending) which creates different risks, as the state is delegating provider contracting, utilization management, and claims processing to a managed care organization (MCO). States with managed care programs have additional program integrity responsibilities.
The federal government’s responsibility is to provide “effective support and assistance to states to combat provider fraud and abuse.” CMS supports states through funding, training, and defining in regulation how states must comply with Medicaid program integrity requirements. Three federal agencies – the HHS Office of Inspector General (OIG), U.S. Department of Justice (DOJ), and Government Accountability Office (GAO) – are also involved in this work, each with different roles and responsibilities. Federal agencies regularly report on Medicaid program integrity performance, including:
- The CMS Improper Payments Fact Sheet, which summarizes and explains annual statistics on HHS improper payment measurements
- The HHS Agency Financial Report, which includes Medicaid payment integrity statistics
- The Payment Error Rate (PERM) Findings and Reports, Supplemental Improper Payment Data Reports2 include state specific data
- The HHS-OIG Healthcare Fraud and Abuse Control (HCFAC) report and the Medicaid Fraud Control Units (MFCU) report, which summarize program integrity oversight and enforcement activities
- GAO’s High-Risk Series identifies government operations with vulnerabilities to fraud, waste, abuse
2. There is no comprehensive or reliable measure of fraud in Medicaid.
Fraud is not unique to Medicaid. Fraud occurs in Medicaid, Medicare, and private health insurance. Most monetary loss from fraud is by providers. Fraud includes obtaining a thing of value through willful misrepresentation. Measuring fraud is difficult, in part, because it can only be determined with certainty after the fact and if it is identified. There are no reliable measures of fraud against Medicaid. DOJ and HHS-OIG operate a Health Care Fraud and Abuse Control (HCFAC) program, designed to coordinate federal, state, and local health care fraud and abuse law enforcement activities. A HCFAC report is published annually, describing health care fraud enforcement actions. Recent analysis of the FY 2023 HCFAC report found no beneficiary fraud in the listing. Providers convicted (of different kinds of fraud against Medicaid and Medicare) included ambulance service providers, durable medical equipment suppliers, diagnostic labs, nursing homes, pain clinics, pharmacies, physical therapists, physicians, and substance use treatment providers. Examples of successful criminal and civil investigations highlighted in the report include:
- Sentencing of an EMT supervisor for an ambulance company who wrote and signed hundreds of false ambulance run sheets that were used to send fraudulent bills to the Texas Medicaid program;
- Sentencing of a pharmacy owner in a scheme to bill Kentucky Medicaid (and other health benefit programs) for drug prescriptions that were never filled; and
- Sentencing of a Michigan physician for his role in a health care fraud scheme that exploited patients suffering from addiction by administering unnecessary back injections and illegally distributing millions of medically unnecessary opioids.
In FY 2023, total HCFAC recoveries reached $3.4 billion (across Medicaid and Medicare). The reported return on investment for the HCFAC program (2021-2023) was $2.80 for every $1 spent. HHS-OIG also publishes an annual summary of the cases brought by state Medicaid Fraud Control Units (MFCUs). The report identifies criminal convictions and civil settlements and judgments by provider type. In FY 2024, MFCUs reported 1,151 convictions and $1.4 billion in recoveries (or $3.46 for every $1 spent).
3. Improper payments are not a measure of fraud.
The Improper Payments Information Act (IPIA) of 2002 (replaced by the Payment Integrity Information Act (PIIA) of 2019) requires the heads of federal agencies to annually review programs they administer and identify those that may be susceptible to significant improper payments, to estimate the amount of improper payments, to submit those estimates to Congress, and to submit a report on actions the agency is taking to reduce the improper payments. The Office of Management and Budget (OMB) has identified Medicaid and CHIP as programs at risk for significant improper payments. As a result, CMS developed the Payment Error Rate Measurement (PERM) program to comply with the IPIA / PIIA and related guidance issued by OMB.
The PERM program measures improper payments in Medicaid and produces a national improper payment rate, which is not a fraud rate. Improper payments, which are often cited when discussing program integrity, are payments that do not meet CMS program requirements. PERM is based on reviews of fee-for-service (FFS), managed care, and eligibility components of a state’s Medicaid program in the year under review. The error rate is not a “fraud rate” (or a waste or abuse rate) but a measurement of payments made that did not meet statutory, regulatory, or administrative requirements or are made in an incorrect amount (including overpayments and underpayments). While fraud and abuse may be one cause of improper payments, not all improper payments represent fraud or abuse. PERM is not designed to detect or measure fraud. States are audited on a rolling three-year basis, meaning each PERM cycle measurement includes one-third of states. Annually, the most recent three cycles are combined to produce a national improper payment rate (weighted by state size). (CMS also produces improper payment rates for CHIP, Medicare, and advanced premium tax credits (APTCs) for the federally facilitated exchange.) As with variation in all aspects of Medicaid operations, PERM rates vary across states ranging from under 1% in Alabama, South Dakota, and Washington to over 20% in South Carolina and Wyoming.
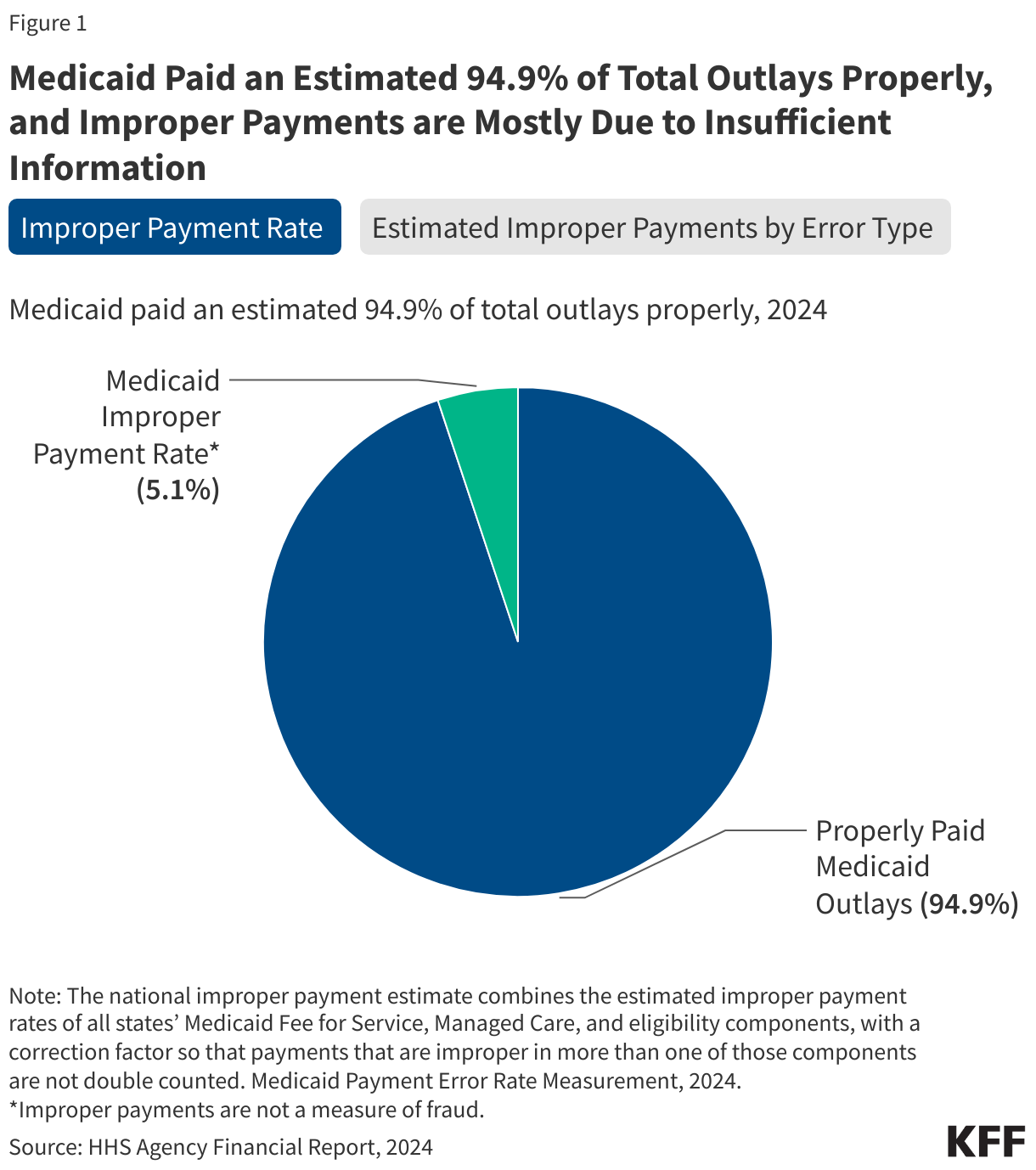
In 2024, Medicaid paid an estimated 94.9% of total outlays properly, representing $579.73 billion in proper federal payments (Figure 1). The overall Medicaid improper payment rate was 5.1% (or $31.10 billion in federal payments). However, 79.1% of the improper Medicaid payments were the result of insufficient documentation or missing administrative steps (Figure 1). These payments were not necessarily for ineligible enrollees, providers, or services (i.e., since they may have been payable if the missing information had been on the claim and/or the state had complied with requirements). Examples include state failure to document beneficiary eligibility or to appropriately screen enrolled providers, or medical records not submitted or missing required documentation to support the medical necessity of a claim. Other improper payments include payments for beneficiaries who were ineligible or were eligible but received a service that was not covered (15.6%), for providers not enrolled in the program (2.0%), and other monetary losses (3.3%) (Figure 1). States are often required to develop and implement corrective action plans for errors and deficiencies.
The 2024 improper payment rate was the lowest rate since the COVID-19 pandemic began due, in part, to flexibilities granted during the public health emergency (e.g., suspended eligibility renewal determinations and reduced requirements for provider enrollment and revalidations) and to improved state compliance with program rules. Prior to the pandemic, the improper payment rate increased following the reintegration of the PERM eligibility component in 2019, which was suspended from 2015 – 2018 to provide states with time to adjust to eligibility process changes in the Affordable Care Act.3 (In its place, CMS required states to implement pilots to assess the accuracy of their eligibility determinations.) While the national improper payment rate increased notably in 2019, 2020, and 2021 (to 21.7%), more than three quarters of improper payments (in each year) were due to insufficient documentation or missing administrative steps (data not shown). In 2024, CMS finalized rules related to eligibility and enrollment that included guidance for states on eligibility documentation procedures to reduce “paperwork” errors that lead to the majority of eligibility-related improper payments. Specifically, the rule requires records to be kept in electronic format for the entire period the case is active and for at least three years after and identifies the information that must be included in all case records; however, Congress may repeal these rules.
4. HHS and CMS identify key areas of program integrity focus, informed in part by recommendations made by other federal agencies.
HHS works with all states to develop strategies to address the root causes of improper payments. States are responsible for implementing, overseeing, and assessing the impact of these strategies and actions. Efforts include systems and process improvements (e.g., adding new claims processing checks, upgrading claims processing systems, and enhancing procedures for provider and beneficiary enrollment).
Every five years, HHS and CMS must issue a comprehensive Medicaid program integrity plan that outlines the agency’s strategy for working with states on program integrity. Historically, program integrity efforts focused on the recovery of misspent funds, but more recent initiatives move beyond “pay and chase” models to focus more heavily on prevention and early detection of fraud and abuse and other improper payments. The FY 2024-2028 CMS plan highlights key areas of focus including Medicaid managed care oversight, eligibility determination processes, systems improvements, data analytics and data sharing, and federal training and technical assistance. To help target oversight activities, CMS will continue to use a risk-based approach to focus efforts on high-risk states, providers, managed care plans, and program areas to maximize return on investment. CMS identified Medicaid managed care, non-emergency medical transport (NEMT), dental benefits, nursing facilities, and home- and community- based services as areas where there may be high-risk program integrity vulnerabilities.
Independent agencies like MACPAC and GAO regularly make recommendations to reduce fraud, waste, and abuse in Medicaid. In 2024, GAO indicated CMS had taken steps to address improper Medicaid payments (consistent with their recommendations) including improving managed care oversight (e.g., increasing audits), assessing fraud risks (including documenting vulnerabilities and identifying mitigation strategies), and improving state compliance with provider screening and enrollment requirements. GAO notes, however, actions on recommendations that remain unimplemented could further enhance program integrity—including additional CMS oversight/action to improve state compliance with provider enrollment and screening requirements, ensure timely state eligibility determinations, and improve collaboration with state auditors. Additionally, GAO made recommendations to CMS about other areas where program oversight and transparency could be improved including managed care, demonstration waivers, and other financing. MACPAC recommendations include simplifying and streamlining program integrity regulatory requirements, improving state-federal coordination, and identifying the most effective program integrity activities.
5. “Fraud, waste, and abuse” are at the forefront of current debates as a basis for making changes in Medicaid and more broadly.
Medicaid is a very complex program that involves millions of beneficiaries, hundreds of thousands of providers, 51 state agencies (including DC), different delivery systems, complicated eligibility rules, and significant federal and state expenditures—all of which together create vulnerabilities and opportunities for error. Since the enactment of Medicaid in 1965, the statute has evolved to promote program integrity. The focus of program integrity efforts has also evolved at CMS in response to changing legislation, policy developments, and priorities. Each administration may approach program integrity differently, with different goals and a willingness to accept different tradeoffs. Republicans in Congress and the Trump Administration state they are not aiming to cut Social Security, Medicare, or Medicaid benefits but aiming to root out fraud, waste and abuse—often citing improper payment estimates as evidence of extensive fraud in Medicaid and Medicare, despite GAO stating improper payments are not designed to identify fraud and are not a measure of fraud or abuse. While policy makers and the public support efforts to root out fraud and make government more efficient, there is little support for broad reductions in federal spending on Medicaid that could affect coverage, benefits, or access to care.
What is known about fraud in Medicaid is that it’s not unique to Medicaid (fraud also occurs in Medicare and private health insurance) and is mostly committed by providers. There are checks on fraud, waste, and abuse at both the federal and the state levels, as described in the sections above. GAO and MACPAC recommendations to reduce fraud and abuse may involve additional investments in oversight and transparency but not reductions in federal funding. As the budget debate continues, there may be efforts to recast certain Medicaid policy changes such as adding work requirements to Medicaid and restricting the use of provider taxes as addressing fraud, waste, and abuse. There are proponents and opponents of such policies, and these policies may come with tradeoffs (e.g., decreasing federal funding while shifting costs to the states and reducing coverage), but they are not about rooting out fraud in Medicaid.
Endnotes
GAO has issued separate overviews that apply government-wide of fraud and improper payments, waste, and abuse.
A subset of states are audited each year; CMS publishes an improper payment rate for the states measured in each cycle – most recently available in 2024 (p. 52), 2023 (p. 52), and 2022 (p. 53).
CMS continued to report the 2014 improper payment rate for eligibility errors as part of its overall PERM improper payment rate calculation.